COMMON SKIN INFECTIONS AMONG SPORTS MEN — A SURVEY
Download PDF
Almost any cutaneous infection can afflict athletes; however, their activities place these individuals at higher risk to develop and subsequently transmit their skin ailment to competitors. Athletes acquire infections as a result of their interaction with other athletes and with the environment in which they compete. An athlete's skin is often macerated from sweating which provides a fertile environment for microorganisms. Furthermore, trauma inherent to sporting activities can create a disturbance in the cutaneous barrier which allows the microorganism to penetrate. Lastly, many sports involve close skin-to-skin contact which facilitates the spread of infectious organisms within and among teams. . The most common infections in sports include bacterial, fungal, and viral infections, but parasites can also afflict the athlete, ( Brian B. Adams ,2008).
COMMON SKIN INFECTIONS AMONG SPORTS MEN -A SURVEY.
B.S.Anuradha * & P.RaviKumar**
* Department of Microbiology Chaitanya Post graduate College Hanamkonda 506001
** Department of Physical Education National Institute of Technology Warangal 506004
INTRODUCTION
Almost any cutaneous infection can afflict athletes; however, their activities place these individuals at higher risk to develop and subsequently transmit their skin ailment to competitors. Athletes acquire infections as a result of their interaction with other athletes and with the environment in which they compete. An athlete's skin is often macerated from sweating which provides a fertile environment for microorganisms. Furthermore, trauma inherent to sporting activities can create a disturbance in the cutaneous barrier which allows the microorganism to penetrate. Lastly, many sports involve close skin-to-skin contact which facilitates the spread of infectious organisms within and among teams. . The most common infections in sports include bacterial, fungal, and viral infections, but parasites can also afflict the athlete, ( Brian B. Adams ,2008).
Athletic participation has increased in popularity in the past several decades. Infectious conditions exemplify the most common cutaneous ailments of athletes. Once infected, athletes may endure loss of practice time and disqualification from competition. Rapid diagnosis, appropriate institution of therapy and attentive prevention programs all minimize the deleterious effects of skin infections for both the athlete and the team. (Adams,2010).
Skin infections account for up to 10% of time-loss injuries in some sports and can cause serious illness. Skin infections can be spread from one athlete to another. We can help protect athletes from becoming sick or losing playing time due to skin infections.
Multiple skin infections in the athlete exist. Fungi, bacteria and viruses cause the majority of sports-related skin infections. Most common skin infections in sports men are Bacterial: Staphylococcal skin infection, Fungal: Dermatophycoses (Ring worm), Viral: Molluscum contagiosum, Herpes simplex, Verruca and Flat worms etc. Several distinct differences in skin infections exist between athletes and nonathletes. (Adams BB, 2006). First, athletes experience a significantly higher prevalence of these infections. As a result of intense skin-to-skin contact, rampant sharing of equipment, occlusive clothing, open wounds and profuse sweating athletes develop and transmit microorganisms at alarming rates. Cutaneous infections cause disruption to an athlete's exercise program by causing discomfort, isolation and disqualification. The basic knowledge about these infections is very important for preventing these infections and also from transmitting them to other players.
Skin infections can lead to:
- Loss of playing time
- Scarring, sometimes on face
- Wounds or rashes that keep recurring
- Rarely, serious life-threatening infections if not treated quickly
This article will discuss the epidemiology, clinical presentation, complications, treatment and prevention of the aforementioned infections in athletes.
Bacterial infections:
Several specific sports-related dermatologic conditions are caused by bacterial infection.(Figure 1). Staphylococcal infection is the most common .(Freeman MJ, Bergfeld WF, 1977, Bergfeld WF, Taylor JS 1985, Sosin DM, Gunn RA, Ford WL, et al ,1989, Powell FC,1994). It causes infections such as impetigo, erysipelas, folliculites,(Freeman MJ,Bergfeld WF,1977, Bergfeld WF, Taylor JS 1985) and furunculosis(Sosin DM, Gunn RA, Ford WL, et al ,1989).These bacterial infections occur in athletes participating in sports in which close personal contact occurs, including rugby, judo, and wrestling. (Brain Adams, 2008) Fomites (bags,mats,balls,bats,towels etc.) also help in transmission of these infections.
Treatment:
Pustules can be treated with topical or oral antibiotics. Isolation of the athlete from others is important to prevent spread of the disease.

Viral skin infections:
Three main viral infections that affect athletes are Verruca (warts), molluscum contagiosum, and herpes simplex.

Treatment:
Destroying Verruca will help to prevent it from growing and possibly causing pain. It also aids in preventing it from spreading. Athletes with Verruca should wear sandals while showering in shared facilities.

Treatment:
Isolation of athletes with infection. The infections should be treated at the earliest by administering anti viral compounds.

Herpes simplex infection ,(figure 4) known as herpes gladiatorum identified in wrestlers, has been reviewed extensively. ( Freeman MJ, Bergfeld WF.1977, Bergfeld WF, Taylor JS.1985 Sosin DM, Gunn RA, Ford WL, et al,1989, . Powell FC.1944, Becker TM 1988, Kodsi R, Bailey P, et al.1998, Becker TM 1992) Herpes simplex infection may also occur in rugby players also.( White WB, Grant-Kels JM 1984) The clinical presentation is that of vesicles on reddish patch on skin. Rupture of these vesicles may result in erosions. Transmission is primarily through skin-to-skin contact.
 -
-
Herpes simplex infections
Treatment:
Identifying infected athletes promptly and excluding them from direct contact with other wrestlers help to halt these infections. Rapid administration of antiviral treatment may accelerate an athlete's return to wrestling.
Fungal infections:
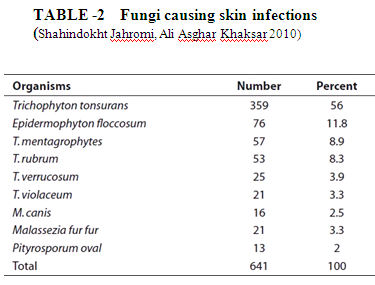
Also known as Dermatophytes, Dermatomycosis, and Ring worm fungi. The common fungal infections are athlete's foot and Jock itch. Athlete's foot or Tinea pedis is commonly seen in runners, skaters, long distant runners, walkers etc.These infections can occur in both hot and cold climates.There are many number of fungi which can cause these infections as seen in table 2.
Tinea pedis (figure 5) mostly occurs in the inter digits of fingers. These are transmitted by direct contact and by fomites especially shoes. Tinea pedis can affect many athletes because the causative organism thrives in warm and moist environments.
Treatment:
Affected athletes should be treated with antifungal agents and also wear protective footwear while using shared facilities to decrease transmission to other athletes.

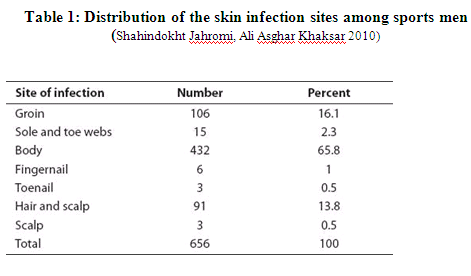
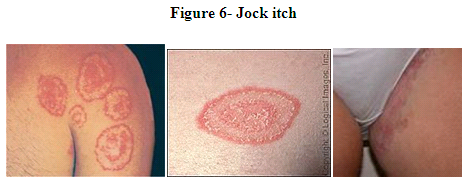
Tinea corporis (figure 6) or Jock itch, dhobi's itch mostly occurs on head, skin and nails. The clinical appearance of tinea corporis gladiatorum varies with the age of the lesion. Mature lesions appear as annular, erythematous, scaling plaques. Mostly seen in wrestlers. Wrestling mats play a large role in transmission.( Vandenesch F, Naimi T, Enright MC et al.2003, Baba T, Takeuchi F, Kuroda M et al 2004)
Treatment:
Athletes, particularly wrestlers and others subjected to extensive skin-to-skin contact should be examined carefully before each practice and competition. Athletes with signs of tinea infection should be treated promptly with antifungal agents and should be removed from direct contact with other wrestlers if the infected area cannot be appropriately covered using bandaging techniques.
Figure 6- Jock itch
Flat worms:
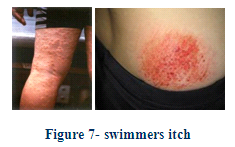
Flat worms mostly cause a infection known as Swimmers itch. Swimmer's itch (figure 8), also known as lake itch,duck itch, cercarial dermatitis, caused by water borne schistosomes. Symptoms, which include itchy, raised papules, commonly occur within hours of infection and do not generally last more than a week.
Treatment:
Orally administered hydroxyzine, an antihistamine, is sometimes prescribed to treat swimmer's itch and similar dermal allergic reactions.
Prevent the spread of infections
Athlete's responsibilities: |
Coaches, Officials, and Team Leaders responsibilities: |
|
|
CONCLUSION
The basic know how about these infections are very important to coaches, managers, and athletes as well. Good hygienic practices should be followed to prevent these infections. Athletes should limit the amount of exposed skin. Fortunately, fabric technology has advanced considerably and athletes can wear long-sleeved clothing that places a barrier between them and their competitors, absorbs the moisture and sweat, and still allows the athlete to regulate their temperature. Infected athletes must meticulously cover their injured skin. During periods of low prevalence of infections in the team and only during practice, trainers may use bandaging techniques on the infected athlete; bandaging alone does not allow one to compete If the infection is severe the athlete should not participate in the event. No athlete should share towels, pads, clothing, razors or protective headgear. After practice and competition, although no supportive evidence exists, athletes should take showers with antibacterial soaps. Furthermore, all clothing and undergarments require daily laundering.
Athletes represent a unique population who acquire skin infections more often than nonathletes. The rapid diagnosis and treatment of these skin infections will prevent disruption to individual training and competition and will minimize epidemics among teams. Frequent, precise and candid communication among the athletes, coaches and medical staff maximizes the potential for a competitive season free from skin infection. Following good hygienic practices is a key element in controlling these skin infections.
REFERENCES:
Adams BB. (2006) Sports Dermatology. Springer, NY, USA .Exhaustive review of cutaneous lesions in athletes.
Baba T, Takeuchi F, Kuroda M et al.,(2002) Genome and virulence determinants of high virulence community-acquired MRSA. Lancet 359, 1819-1827).
Becker TM, Kodsi R, Bailey P, et al.(1988), Grappling with herpes: herpes gladiatorum. Am J Sports Med;16: 665-669.
Becker TM(1992). Herpes gladiatorum: a growing problem in sports medicine. Cutis 50: 150-152.
Belongia EA, Goodman JL, Holland EJ, et al.,(1991) An outbreak of herpes gladiatorum at a high-school wrestling camp. N Engl J Med;325: 906-910: 906-910. Bergfeld WF, Taylor JS. (1985). Trauma, sports, and the skin. Am J Ind Med;8: 403-413.
Brian B. Adams, MD, MPH (2008) ,Dermatology Nursing. 20(1):39-44. © 2008 Jannetti Publications, Inc.
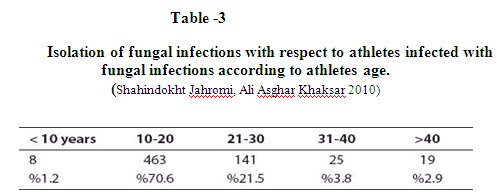
Shahindokht Bassiri-Jahromi , Ali Asghar Khaksar (2010) Prevalence of cutaneous fungal infections among sports-active individuals . 2010, 3: 2 : 53-57. |
Freeman MJ, Bergfeld WF(1977). Skin diseases of football and wrestling participants. Cutis ;20: 333-341.
Powell FC.(1994). Sports dermatology. J Eur Acad Dermatol Venereol 3: 1-15.
Sosin DM, Gunn RA, Ford WL, et al.,(1989). An outbreak of furunculosis among high school athletes. Am J Sports Med 17: 828-832.
White WB, Grant-Kels JM.(1984) Transmission of herpes simplex virus type 1 infection in rugby players. JAMA;252: 533-535.
Skin diseases of football and wrestling participants. Cutis. 1977 Sep; 20(3):333-41.
ReviewHerpes gladiatorum: a growing problem in sports medicine. Cutis. 1992 Aug; 50(2):150-2.
Transmission of herpes simplex virus type 1 infection in rugby players. JAMA. 1984 Jul 27; 252(4):533-5.
Vandenesch F, Naimi T, Enright MC et al. Community-acquired methicillin-resistant Staphylococcus aureus carrying Panton-Valentine leukocidin genes: worldwide emergence. Emerg. Infect. Dis. 9, 978-984 (2003).
















